Description of the Situation
GLOBAL OVERVIEW
Current Situation
Since 2021, there has been an increase in cholera cases and their geographical distribution globally. In 2021, 23 countries reported cholera outbreaks, mainly in the WHO Regions of Africa and the Eastern Mediterranean. This trend has continued into 2022 with over 29 countries (Figure 1) reporting cholera cases or outbreaks. As of 30 November 2022, 16 of these have been reporting protracted outbreaks. Many of those countries reported higher case numbers and case fatality ratio (CFR) than in previous years. The average cholera CFR reported globally in 2021 was 1.9% (2.9% in Africa), well above acceptable (<1%) and the highest recorded in over a decade.
This year the number of cholera cases and cholera-associated deaths have surged globally following years of decline. Of particular concern are the outbreaks in 13 countries, which did not report cholera cases in 2021. Of these, some had not reported any cholera outbreaks for many years (between three and 30), and several are not considered cholera-endemic countries.i,ii The current situation represents a resurgence of the ongoing seventh pandemic of cholera which began in 1961.
The simultaneous progression of several cholera outbreaks, compounded in countries facing complex humanitarian crises with fragile health systems and aggravated by climate change, poses challenges to outbreak response and risks further spreading to other countries. The overall capacity to respond to the multiple and simultaneous outbreaks is strained due to the global lack of resources, including the oral cholera vaccine, as well as overstretched public health and medical personnel, who are often dealing with multiple disease outbreaks at the same time.
 Note: countries in white did not report any cholera cases in 2022
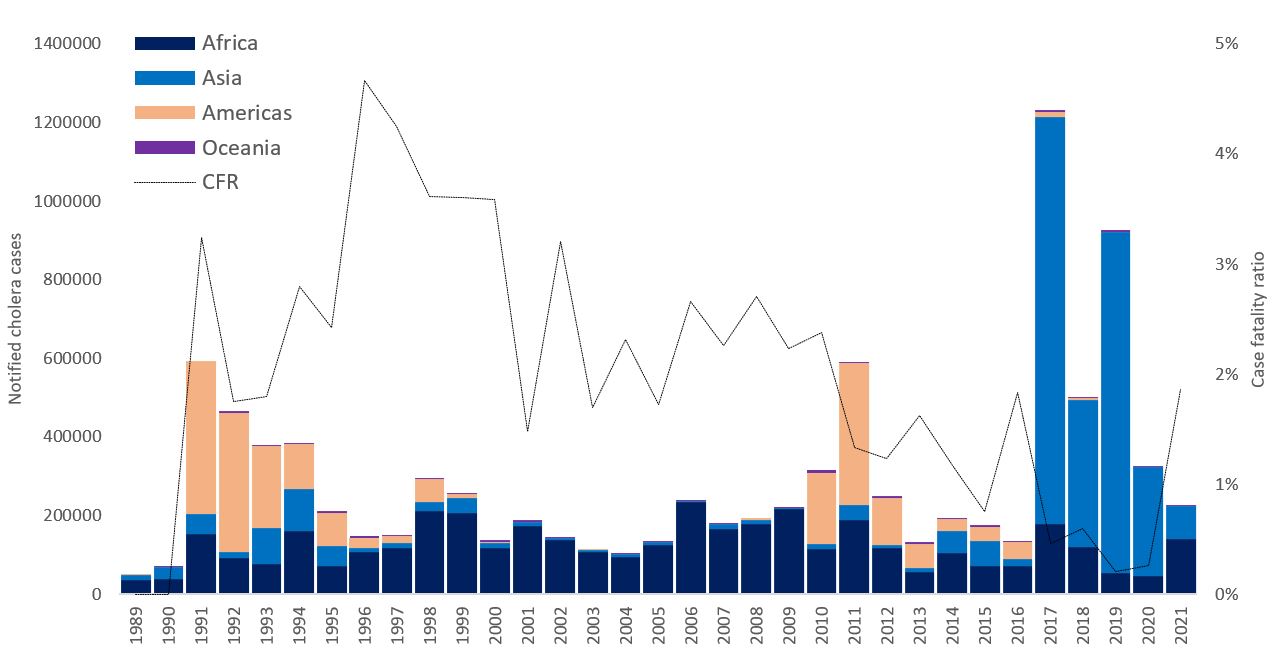
Note: countries in white did not report any cholera cases in 2022 Figure-2: Cholera cases* reported to WHO by year and continent, global CFR, 1989-2021**
DRIVERS OF THE CURRENT OUTBREAKS AND CHALLENGES IMPACTING THE RESPONSE
The main drivers and challenges for controlling and containing the current cholera outbreaks are outlined below. Yet, addressing the need for, and lack of funding to prevent outbreaks is critical. Large-scale investments in water and sanitation infrastructure have largely led to the elimination of cholera in Europe and the Americas. Significant investments should support water, sanitation, and hygiene (WASH) interventions for cholera prevention and control. Such interventions should consider the social context and be supported by the best available evidence and updated models of cholera transmission.1
- Climate change – widespread floods and drought
Of the countries that have reported cholera outbreaks in 2022, many are experiencing natural disasters such as cyclones (Mozambique, Malawi), flooding (Pakistan, Nigeria), and drought (countries in the Horn of Africa). Major flooding and above-normal hurricane seasons increase outbreak severity and the propensity for regional spread. The upcoming rainy/cyclone season, which is predicted to be severe, has the potential to spread the disease across Southern Africa. The above-normal hurricane season in the Americas is affecting several countries in the Caribbean and Central America causing major flooding. Post-monsoon season (and post-floods) is usually associated with a cholera peak in South Asia. Additionally, many countries experienced droughts leading to cholera2 due to poor access to water, marginalization of refugees and nomadic populations, and expansion of informal urban settlements.
- Humanitarian crises, political instability, and conflict
Increasing humanitarian crises due to conflict, political instability, and a lack of development are leaving an increasing number of people at risk for cholera across all WHO regions. Of the countries that have reported outbreaks, nine are experiencing conflict or political violence in affected areas (Afghanistan, Cameroon, the Democratic Republic of Congo, Haiti, the Islamic Republic of Iran, Nigeria, Somalia, the Syrian Arab Republic, and Yemen). In two of these countries (Ethiopia and Cameroon), the current outbreak is not affecting conflict areas, but there is a high risk of spreading into areas of ongoing conflict, which would complicate the response.
- Multiple ongoing emergencies
Several countries with cholera outbreaks are also responding to multiple other disease outbreaks including mpox (monkeypox), dengue, chikungunya, measles, and the ongoing COVID-19 pandemic. This also strains the overall response capacity to cholera, particularly in countries with limited resources.
- Sub-optimal / delayed surveillance.
The lack of data hinders response. There are several country- and surveillance-specific reasons for the lack of data: (1) Countries with inadequate surveillance systems overall; (2) Countries with robust surveillance systems, which only report cholera from sentinel sites or do not include cholera at all; (3) Lack of data sharing; (4) Breakdown of surveillance systems during humanitarian crises and political instability; (5) Insufficient capacity for lab confirmation and use of heterogenous case definitions (eg. cholera versus acute watery diarrhea).
- Medical commodities supply chain
At the time of this report, the global supply of cholera kits is depleted, and suppliers are struggling to meet demand. Delays or shortages of medical supplies can lead to preventable and avoidable deaths. WHO is facilitating global coordination and alternate sources of supply are being sought, but these will not be available immediately.
- Limited availability of healthcare resources
The number of outbreaks and geographic scope has stretched the capacity of healthcare services to implement a comprehensive multisectoral response. Parallel large-scale, high-risk outbreaks and other public health and humanitarian crises are further stretching resources and limiting the capacity to respond. In addition, the emigration of skilled medical personnel during a humanitarian crisis, interruption in routine health services such as vaccination leading to (re)-emergence of vaccine-preventable diseases, destruction or inaccessibility of healthcare infrastructure, and violence against health workers have hindered outbreak response activities.
- Availability of oral cholera vaccine
The global stockpile of Oral Cholera Vaccine (OCV) is currently insufficient to meet all requests for two doses of preventive vaccination. As a result, on 20 October 2022, the International Coordinating Group (ICG) members (IFRC, MSF, UNICEF, and WHO) took the unprecedented decision to temporarily limit all reactive OCV campaigns to one single dose. The production of OCV is a continuous process with around 2.5 million doses produced monthly. As vaccine manufacturers are producing at their maximum current capacity, there is no short-term solution to increase production. While using a single dose instead of two doses will allow more people to be protected in the short term, this strategy has its limitations, and it is unclear how long immunity will last. To solve the problem in the long term there needs to be an increase in global vaccine production. Since the creation of the global stockpile in 2013, more than 50 million doses of OCV have been successfully used in various settings through mass campaigns.3
REGIONAL OVERVIEW
In the table below, some countries under monitoring are described. These include countries with recently reported outbreaks of cholera, countries where we have observed a continuous rise in cases with challenges to control the outbreak, countries with protracted outbreaks with challenges to control, countries with repeated outbreaks in 2022, countries with large vulnerable populations, and countries where insecurity and conflict hinder the response.
Epidemiology
Cholera is an acute diarrheal infection characterized, in its severe form, by extreme watery diarrhea and potentially fatal dehydration. It is caused by the ingestion of food or water contaminated with the bacterium Vibrio cholerae. It has a short incubation period, ranging between two hours and five days. Most people will develop no or only mild symptoms; less than 20% of ill persons develop acute watery diarrhoea with moderate or severe dehydration and are at risk for rapid loss of body fluids, dehydration, and death. Despite being easily treatable with rehydration solution, cholera remains a global threat due to its high morbidity and mortality in vulnerable populations with a lack of access to adequate health care.
Seven distinct pandemics of cholera have been recorded during the past two centuries. The seventh pandemic, which is still ongoing today, is considered to have occurred principally between 1961 to 1974. During this period, following (re)introduction, many countries transitioned to becoming cholera-endemic. While global incidence greatly decreased in the late 1990s, cholera remained prevalent in parts of Africa and Asia.
The global burden of cholera is largely unknown because the majority of cases are not reported, however, previous studies estimate 2.9 million cases, and 95,000 deaths occur annually.
Public Health Response
WHO is working with partners at global, regional & country level to support Member States in the following cholera outbreak response activities:
Coordination
- Providing a forum for technical expertise exchange through the Global Task Force on Cholera Control (GTFCC) coordination, and cooperation on cholera-related activities to strengthen the country’s capacity to prevent and control cholera.
- Providing technical support to all ongoing outbreaks (laboratory, case management, OCV, WASH).
- Collaborating with key partners (UNICEF, MSF) to coordinate supply and optimal access to supplies.
- Leveraging resources to support global monitoring of the cholera pandemic, provide technical support to countries, enhance data collection and reporting, strengthen advocacy, and provide medical and non-medical items to countries in need, especially for case management and diagnosis.
- Supporting the deployment of experts through GAVI, GOARN, and standby partners.
Surveillance
- Strengthening surveillance including strengthening diagnostic algorithms, use of rapid diagnostic tests, collecting and transporting of samples, and strengthening laboratory capacity to culture V. cholerae.
Vaccine
- Providing guidance to identify target populations for vaccination and requesting vaccine through the ICG mechanism, in the context of acutely limited supply.
- Supporting advocacy to increase OCV production and engage new vaccine manufacturers.
- Working with countries to identify the areas/hotspots where vaccination is most needed.6
Case management
- Strengthening case management and improving access to treatment for patients by setting-up dedicated healthcare facilities (Cholera Treatment Centres (CTCs) and Cholera Treatment Units (CTUs)) and training health workers and provision of technical guidance
Infection Prevention and Control (IPC)
- Conducting advocacy and resource mobilization activities to support cholera prevention and control at national, regional, and global levels.
Risk communication and community engagement (RCCE)
- Working closely with Member States and partners to strengthen risk communication and community engagement plans and strategies, adapted to local beliefs and contexts, to encourage behavioural change and adoption of appropriate protective measures such as vaccination, and ensuring safe food, water, and hygiene practices.
- Providing support to increasing risk perception and knowledge among communities about the disease, its symptoms, associated risks, precautions to take, and when to seek treatment when symptoms appear.
Water, Sanitation, and Hygiene (WASH)
- Working closely with Member States and partners to strengthen water, hygiene, and sanitation systems through multi-sectoral mechanisms, including IPC and guidance on water quality monitoring.
- Supporting countries for the implementation of effective cholera control strategies and monitoring of progress.
Operations, Support, and Logistics (OSL)
- Working closely with suppliers to secure Cholera Kits, sourcing other WASH supplies, and establishing a pipeline for bulk items.
WHO Risk Assessment
On 26 October 2022, WHO assessed the risk of cholera at the global level as very high, remaining a global threat to public health and an indicator of inequity and lack of social development. There has been an increase in global reported cholera outbreaks with 29 countries, mainly in the WHO African and Eastern Mediterranean Regions, reporting outbreaks to WHO in 2022 with many of those reporting higher case numbers and case fatality ratios (CFR) than in previous years.
Several countries are in the midst of complex humanitarian crises with fragile health systems, inadequate access to clean water and sanitation, and insufficient capacity to respond to these outbreaks. Climate change and lack of development also contribute to outbreaks, and cross-border population movements. The latter, along with increased global travel following the COVID-19 pandemic, further increase the risk of international spread.
The number of outbreaks occurring simultaneously across all WHO Regions is straining the overall epidemic response capacity. Protracted outbreaks of cholera are draining public health response personnel and depleting resources.
Due to the global shortage of OCV, the ICG recently made the unprecedented decision to temporarily suspend the second dose strategy for the outbreak response. There are also significant delays and shortages of medical supplies that can lead to preventable and avoidable deaths.
WHO Advice
WHO recommends improving access to proper and timely case management of cholera cases, improving access to safe drinking water and sanitation infrastructure, as well as improving infection prevention and control in healthcare facilities. These measures along with the promotion of preventive hygiene practices and food safety in affected communities are the most effective means of controlling cholera. Effective risk communication and community engagement strategies are needed to encourage behavioral change and adoption of appropriate preventive measures.
The OCV should be used in conjunction with improvements in water and sanitation to control cholera outbreaks and for prevention in targeted areas known to be at high risk for cholera.
WHO recommends Member States to strengthen and maintain surveillance for cholera, especially at the community level, for the early detection of suspected cases and to provide adequate treatment and prevent its spread. Early and adequate treatment limits the CFR of patients to less than 1%.
WHO does not recommend any travel or trade restrictions on Member States based on the currently available information. However, as the outbreak also affects border areas where there is a significant cross-border movement, WHO encourages Member States to ensure cooperation and regular information sharing across all levels of the organization so that any spread across the border is quickly assessed and contained.
Further Information
- Disease outbreak news Cholera - Haiti
- Disease outbreak news Cholera – Cameroon
- Disease outbreak news Cholera - Malawi
- Disease outbreak news Cholera - Lebanon
- Disease outbreak news Cholera - Somalia
- Disease outbreak news Cholera - Pakistan
- ENDING CHOLERA, A GLOBAL ROADMAP TO 2030
- Cholera fact sheet
References
- D’Mello-Guyett, L., Gallandat, K., Van den Bergh, R., Taylor, D., Bulit, G., Legros, D., Maes, P., Checchi, F., Cumming, O., 2020. Prevention and control of cholera with household and community water, sanitation and hygiene (WASH) interventions: A scoping review of current international guidelines. PloS One 15, e0226549. https://doi.org/10.1371/journal.pone.0226549
- Full article: Drought-related cholera outbreaks in Africa and the implications for climate change: a narrative review [WWW Document], n.d. URL https://www.tandfonline.com/doi/full/10.1080/20477724.2021.1981716 (accessed 12.12.22).
- Ali, M., Nelson, A.R., Lopez, A.L., Sack, D.A., 2015. Updated Global Burden of Cholera in Endemic Countries. PLoS Negl. Trop. Dis. 9, e0003832. https://doi.org/10.1371/journal.pntd.0003832
- Cholera Haiti - Risk assessment - PAHO/WHO | Pan American Health Organization [WWW Document], n.d. URL https://www.paho.org/en/documents/cholera-haiti-risk-assessment (accessed 12.15.22).
- Cholera- Haiti [WWW Document], n.d. URL https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON427 (accessed 12.15.22).
- About the International Coordinating Group (ICG) on Vaccine Provision [WWW Document], n.d. URL https://www.who.int/groups/icg/about (accessed 12.12.22).
Citable reference: World Health Organization (16 December 2022). Disease Outbreak News; Cholera – Global situation. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON426